Research Highlights
New Study Finds that ALS and MS Likely Share an Environmental Cause
—

Research finds a phenomena that may have been previously masked by the data
A new study published in Nature’s Scientific Reports indicates that amyotrophic lateral sclerosis (ALS) and multiple sclerosis (MS) have an extremely high geographic association, even after controlling for race, gender, wealth, latitude, and access to neurological healthcare.
“The results of the study are surprising because previous studies have typically concluded there was no evidence for a mechanistic or genetic link between the two diseases,” explains NYU Stern Professor and study author Melissa Schilling, who specializes in analyzing large-scale datasets using econometrics.
Heat maps in accompanying Figure 1 show the geographic patterns of the diseases in the US.
Figure 1: Age-Adjusted Crude Rates in the U.S., by state, 2018 - 2022, People Characterized as "White, Non-Hispanic or Latino" from CDC WONDER database
a) ALS
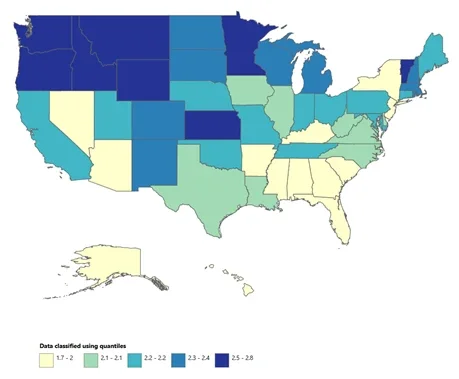
b) MS
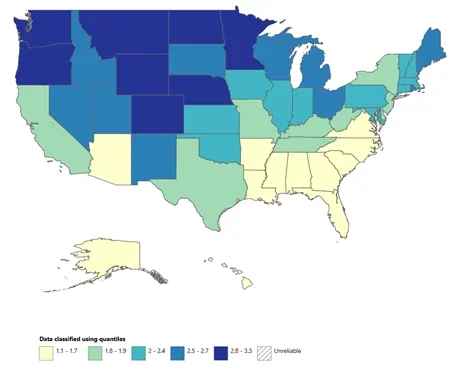
Source: Figure reproduced from Schilling, MA 2025. The geographic association of multiple sclerosis and amyotrophic lateral sclerosis. Scientific Reports, October 14th. Figure based on data from the U.S. CDC Wonder database.
The study also shows that the relationship between the two diseases has likely been overlooked until now because of a “Simpson’s Paradox”—a statistical phenomenon whereby a trend appears in different groups of data but disappears or reverses when the groups are combined.
In this case, the groups are based on gender: As shown in accompanying Figure 2, both women and men show a strong positive correlation (greater than 70 percent) in the geographic distribution of ALS and MS, but when the data are pooled across gender, these relationships are obscured because, on average, ALS is more common in men and MS is more common in women.
Figure 2: Scatterplot of ALS and MS age-adjusted crude rates using CDC WONDER Multiple Cause Data on "White, Non-Hispanic or Latino origin" only, by Gender
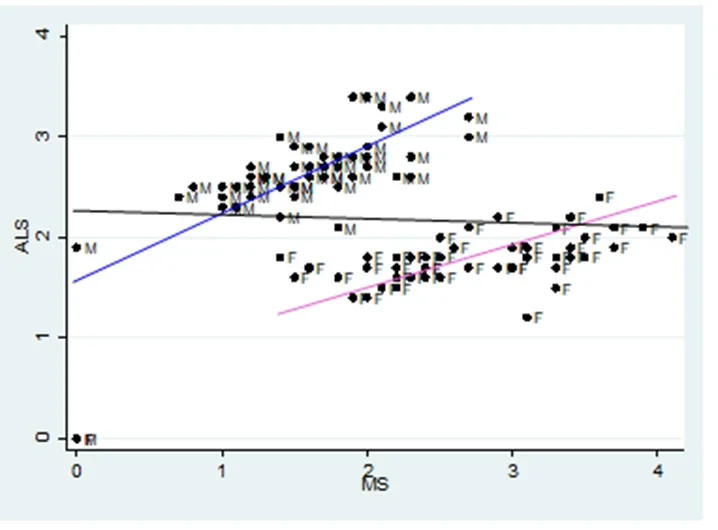
Source: Figure reproduced from Schilling, MA 2025. The geographic association of multiple sclerosis and amyotrophic lateral sclerosis. Scientific Reports, October 14th. Figure based on data from the U.S. CDC Wonder database.
For several decades researchers have noted a north-south gradient in the distribution of MS. This led to speculation that UV light or vitamin D might play a role in the disease, but studies that supplemented MS patients with UV light or vitamin D had minimal or inconsistent results.
The findings in the new Scientific Reports study indicate that MS and ALS have a much stronger geographic relationship with each other than with latitude, suggesting that both diseases may share a connection to a factor that varies imperfectly with latitude.
“I started gathering and analyzing every dataset I could find relevant to ALS about nine years ago when a friend with ALS asked me if I would take a look at the data,” says Schilling. “I was very surprised to find such a strong geographic pattern as most of the research on ALS does not emphasize the role of geography. I was even more surprised to find that ALS has a very strong association with the geography of MS.
“This finding is important because it suggests that an environmental factor likely plays a significant role in both diseases, and that could provide clues that help us determine what causes them and how they might be avoided or treated.”
Elements of the environment that vary imperfectly with the north-south gradient include natural things like viruses, parasites, algae, and molds, as well as human-made elements or practices like the use of heating oil, agricultural practices, industrial practices, mining, and chemical contamination of fisheries.
“The list of suspects is long, but comparing across geographies and, in particular, across outlier locations, such as the Faroe Islands, where MS increased strikingly after military troops arrived there in the 1940s, could significantly narrow the hunt,” observes Schilling.
The study combined mortality and demographic data obtained from the US Centers for Disease Control and Prevention WONDER database (in the US, the collection of mortality data is mandatory and standardized) with latitude data, economic data, and data on access to neurological healthcare. The primary results are based on US crude mortality rates at the state level. The analysis was then replicated at the global level using mortality data from the World Health Organization and obtained nearly identical results.